Background and potential as a bioweapon
Smallpox is caused by the variola virus (VARV), a member of the Orthopoxvirus (OPV) genus of the Poxviridae. In the past, the disease was named smallpox because the lesion size was smaller than great-pox (syphilis) (Meyer et al. 2020).
Widespread vaccination programs were responsible for the global eradication of smallpox, which was certified by the World Health Organisation (WHO) on May 8, 1980. The last person to die from smallpox was Janet Parker, a medical photographer at England’s Birmingham University Medical School. Janet Parker died on September 11, 1978 (CDC. History of Smallpox. n.d.).
Although smallpox has been eliminated from its human reservoir, viable variola virus (VARV) is kept in two maximum security laboratories, one in Russia and the other in the U.S. Unfortunately, the 2001 intentional release of anthrax genetically similar to samples held under the control of the U.S. Department of Defense (DoD) has demonstrated that even the highest biohazard security is fallible.
Beside a possible breach of the repositories in Russia and the U.S., other possible threats by malicious actors have been recognized:
Historical Example of Smallpox Weaponization The weaponization of smallpox in the American colonies during the 1700s is recorded in communications from Sir Jeffrey Amherst, the British Commander-in-Chief of the Forces in North America during the French and Indian Wars. Sir Jeffrey Amherst wrote "Could it not be contrived to Send the Small Pox among those Disaffected Tribes of Indians? We must, on this occasion, Use Every Stratagem in our power to Reduce them.” and "as well as try Every other method that can serve to Extirpate this Execreble [sic] Race.” Probably unknown to Sir Amherst, the colonial trader William Trent had already written in his diary that he had gifted two blankets and a silk handkerchief to emissaries of the enemy Native American tribes. Trent knew the gifts had been used by smallpox-infected colonists. Trent later asked for reimbursement for the blankets and handkerchief, which was approved by the British military. Smallpox was rampant in the North American colonies at that time, so it is likely that decimation of the tribes was inevitable, but the intent and the opportunity to use smallpox as a weapon have been documented (Kiger, 2018). |
The threat to the U.S. is far greater today because routine vaccination ended in the U.S. more than 25 years ago; as a result, the vast majority of our highly mobile population is without any immunity and is highly susceptible. Today's transportation systems could spread smallpox quickly throughout the world. The CDC states "Even a single confirmed case of smallpox today would be considered an emergency" (CDC. The Threat. n.d.).
Instant Feedback:
Recombinant Variola virus could be engineered and produced by malicious actors .
|
| The last known person in the world to have smallpox of any kind. Here 23-year-old Ali Maow Maalin of Merka, Somalia exhibits the pox of Variola minor. |
Transmission
A modern weaponized airborne form of smallpox could be transmitted to a vast numbers of people before the etiology and scale of the contagion would be identified. It is expected that the death rate from an aerosolised smallpox weapon would be higher today than previous epidemics because:
Instant Feedback:
Due to the fact that most of the world’s population has no immunity to smallpox, the human cost of smallpox terrorism could be higher than any previous epidemics.
Smallpox is highly contagious. The variola virus spreads from person to person primarily by droplet nuclei or aerosols expelled from the throat of infected persons and by direct contact. Contaminated clothing or bed linens can also spread the virus. Historically, the seasonal occurrence of smallpox is similar to that of chickenpox and measles – with incidence higher in winter and spring. The infectious dose is unknown, but is believed to be only a few virons. In the 1960’s and 1970’s in Europe, during a very limited smallpox outbreak, individuals with the infection transmitted smallpox to as many as 10 to 20 other people. 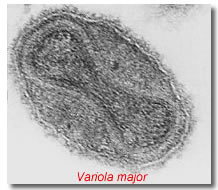 The virus that causes smallpox occurs in two predominant strains – variola major(right), which has a 30% or greater mortality rate, and variola minor, with a 1% mortality rate. Hemorrhagic smallpox and malignant smallpox are two rare but deadly strains of the disease. Before the introduction of smallpox vaccination, almost everyone eventually developed smallpox, and either died of it or developed immunity.
The virus that causes smallpox occurs in two predominant strains – variola major(right), which has a 30% or greater mortality rate, and variola minor, with a 1% mortality rate. Hemorrhagic smallpox and malignant smallpox are two rare but deadly strains of the disease. Before the introduction of smallpox vaccination, almost everyone eventually developed smallpox, and either died of it or developed immunity.
Instant Feedback:
Due to the fact that most of the world’s population has no immunity to smallpox, the human cost of smallpox terrorism could be higher than any previous epidemics.
Smallpox, as a disease, was relatively easy to recognize with its characteristic skin lesions, however, the following exanthematous diseases have to be considered as differential diagnosis: severe chickenpox rash, monkeypox, generalized vaccinia virus or cowpox virus infections an several others. (Meyer et al. , 2020).
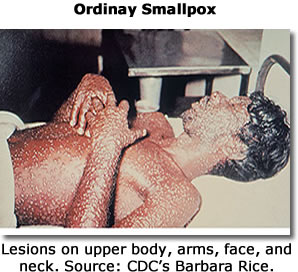
The incubation period of smallpox ranges from 7 to 17 days, with an average length of time between exposure and symptom development of 12 to 14 days. The patient then typically develops a high fever, malaise, and prostration, with headache and backache. Severe abdominal pain and delirium are sometimes present. A maculopapular rash then appears on the mucosa of the mouth and throat, and the face and forearms, and spreads to the trunk and legs. A person with smallpox is sometimes contagious with onset of fever (prodrome phase), but the person becomes most contagious with the onset of rash. The lesions that first appear in the mouth and throat release large amounts of virus into the saliva. Smallpox pustules are characteristically round, hard, and deeply embedded in the dermis. Crusts begin to form on about the eighth or ninth day of the rash. As the patient recovers, the scabs separate and pitted scars develop, primarily on the face.
Instant Feedback:
Patients with smallpox can transmit the disease before the rash appears
Ordinary smallpox was the most common form, accounting for over 85% of all cases during the smallpox era. |
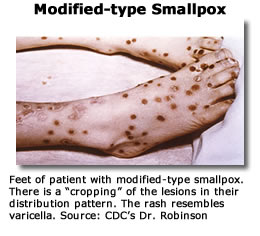
Modified-type smallpox occurs in previously vaccinated individuals. May also be fewer, more superficial lesions than those seen in ordinary smallpox. Patients also do not tend to have a fever during the evolution of the rash. |
Very rare, and is characterized by intense toxemia, majority of flat-type smallpox cases are fatal. If the patient survives, the lesions gradually disappear without forming scabs |
More common in adults and pregnant women. Death usually occurs by the 5th or 6th day of the rash, often before characteristic smallpox lesions develop. Death results from a profound toxemia, leading to multi-organ failure. |
Treatment
Treatment of smallpox patients generally involves supportive care.
Controlling an epidemic – detection, isolation, surveillance, and selective vaccination
A smallpox outbreak poses difficult public health problems because of the ability of the virus to continue to spread throughout the population unless checked by vaccination and/or isolation of patients and their close contacts. Early detection, isolation of infected individuals, surveillance of contacts, and a focused selective vaccination program are the essential elements of a smallpox control program. As soon as the diagnosis of smallpox is made, all persons who are suspected of being infected with smallpox should be immediately isolated and all contacts should be vaccinated and placed under surveillance. It is recommended that contacts be defined as persons who have been in the same household as the infected individual or who have been in face to face contact with the patient after the onset of fever.
Because the widespread dissemination of smallpox virus by aerosol poses a serious threat in hospitals, patients should be isolated at home or in other non-hospital facilities whenever possible. During the worldwide eradication campaign, investigations showed that smallpox was spread throughout hospitals via ventilation systems. Hospital acquired infections may be acquired as a result of droplets spread from patients to staff and visitors in reasonably close contact or by a fine particle aerosol.
In one situation in Germany, a smallpox patient with a cough, who was isolated in a single room, infected persons on 3 separate floors of the hospital. A number of outbreaks have also occurred in laundry workers who handled linens and blankets used by patients. It is recommended in an outbreak setting that all hospital employees as well as patients in the hospital be vaccinated. For persons who are immunocompromised or for whom vaccine is otherwise contraindicated, vaccine immune globulin (VIG) can be given as an alternative.
Instant Feedback:
Patients with smallpox can transmit the disease before the rash appears
If a large outbreak occurs, patients who have active smallpox infections may be quarantined. Although cooperation by most patients and contacts in observing isolation could be ensured through counseling and persuasion, there may be some for whom forcible quarantine will be required. Some states and cities in the U.S., but not all, confer broad discretionary powers on health authorities to ensure the safety of the public’s health and at one time this included powers to quarantine. Under epidemic circumstances, this could be an important power to have. In larger outbreaks, home isolations and care should be the objective for most patients.
Care
Caregivers must practice strict infection control measures in caring for a patient with smallpox in the home. All contaminated instruments, surfaces, excretions, fluids, and other materials should be incinerated or decontaminated chemically. Clothing and bedding should be incinerated, autoclaved, or washed in hot water and hypochlorite bleach.
Pre–exposure vaccination
Before 1972, smallpox vaccination was recommended for all U.S. children at age 1 year. Most states required that each child be vaccinated before school entry. Routine vaccination in the U.S. stopped in 1972 and since then, few persons younger than 27 have been vaccinated. According to the U.S. Census Bureau, in 1998, 42% of the U.S. population was 29 years or younger. The immune status of those who were vaccinated before smallpox vaccination ceased is not clear, as the length of immunity has never been satisfactorily measured. Neutralizing antibodies have been shown to decline substantially during a 5 to 10-year period. Thus, even those who received the recommended single dose vaccination as children do not have lifelong immunity. Because comparatively few persons today have been successfully vaccinated on more than 1 occasion, it must be assumed that the population at large is highly susceptible to infection.
Instant Feedback:
Patients with smallpox can transmit the disease before the rash appears
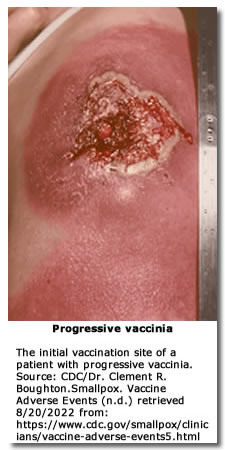 There are some risks associated with smallpox vaccination. Complications of smallpox vaccination include postvaccinal encephalitis, progressive vaccinia – a condition in which the vaccination lesion fails to heal. Additionally, can involve other body tissues, and accidental inoculation of other body parts such as the eyes or mouth, usually by scratching the smallpox vaccination site.
There are some risks associated with smallpox vaccination. Complications of smallpox vaccination include postvaccinal encephalitis, progressive vaccinia – a condition in which the vaccination lesion fails to heal. Additionally, can involve other body tissues, and accidental inoculation of other body parts such as the eyes or mouth, usually by scratching the smallpox vaccination site.
People considered to be at particular risk of smallpox vaccine complications include:
Vaccinia immune globulin (VIG) may be given as an alternative to patients in high-risk groups. VIG may also be given to treat patients with progressive vaccinia. Because the availability of VIG is limited, its use should be reserved for the most serious cases. The U.S. government is working with manufacturers to produce additional doses of smallpox vaccine. To control a smallpox epidemic, it is likely that selective focused vaccination would be used rather than a mass vaccination program. It is important for health care professionals to explain to the lay public why selective vaccination rather than widespread vaccination may be used to control a smallpox epidemic.
Instant Feedback:
Selective vaccination, rather than mass vaccination, would be the strategy most likely used to control a smallpox epidemic.
Vaccination given within the first few days after exposure to a person with smallpox may prevent or lessen smallpox symptoms. Should a smallpox outbreak occur, an emergency vaccination program would be implemented. The vaccine program would include all health care workers at clinics or hospitals that might receive patients, all other essential disaster response personnel, such as police, firefighters, public health and emergency personnel and mortuary staff who might have to handle bodies. Both airborne and contact precautions should also be used in postmortem care. Whenever possible, patients who die of smallpox should be cremated.
Instant Feedback:
Selective vaccination, rather than mass vaccination, would be the strategy most likely used to control a smallpox epidemic.
References
Brown, L. (2014). Smallpox Preparedness Planning: Understanding the Strategic National Stockpile and Potential Weaponization. National Association of County and City Health Officials (NACCHO). Retrieved 8/20/2022 from https://www.naccho.org/blog/articles/smallpox-preparedness-planning-understanding-the-strategic-national-stockpile-and-potential-weaponization
CDC/Dr. Clement. R. Boughton (.n.d.). Smallpox. Vaccine Adverse events. Retrieved 8/20/2022 from: https://www.cdc.gov/smallpox/clinicians/vaccine-adverse-events5.html
CDC. Smallpox. History of Smallpox. (n.d.) retrieved on 8/21/2022 from https://www.cdc.gov/smallpox/history/history.html
CDC. Smallpox. The Threat. (n.d.). Retrieved 8/20/2022 from https://www.cdc.gov/smallpox/bioterrorism/public/threat.html
CDC. Smallpox. Treatment. (n.d.). Retrieved 8/20/2022 from https://www.cdc.gov/smallpox/clinicians/treatment.html
Kiger, P. J. (2018, November 15). Did colonists give infected blankets to Native Americans as biological warfare? History.com. Retrieved August 17, 2022, from https://www.history.com/news/colonists-native-americans-smallpox-blankets
McClain, D. (1997) Chapter 27 smallpox - globalsecurity.org. Retrieved August 20, 2022, from https://www.globalsecurity.org/wmd/library/report/1997/cwbw/Ch27.pdf