|
Differentiation of AOM from OME is essential to developing an effective treatment plan. |
|




Instant feedback
© RnCeus.com
Statistics support the presumption of OME when an infant or toddler presents with otalgia or hearing loss following an upper respiratory infection. However, diagnosing OME requires evidence of fluid within the ME. Evidence of ME fluid can be obtained either indirectly or directly.
Indirect evidence
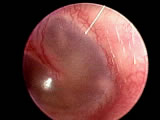
The standard procedure for determining the status of the ME is to observe the TM for integrity, color, clarity, and mobility. Visualization of the TM with a pneumatic otoscope is strongly recommended as a means of determining if there is fluid in the ME. Fluid or pus in the ME will restrict movement of the TM. To assess this, the provider applies gentle pressure via the pneumatic otoscope. The TM should move briskly with the application of slight positive and negative pressure.
Tympanometry is an additional confirmatory test which, when used in conjunction with pneumatic otoscopy, can improve the accuracy of diagnosis. Tympanometry is an objective test that measures the amount of sound energy absorbed by the TM. It evaluates TM movement under positive and negative pressure; little or no movement can indicate fluid in the ME.
Direct evidence
Tympanocentesis and myringotomy are two direct means of determining the presence of ME fluid. Both tympanocentesis and myringotomy are invasive procedures. Tympanocentesis is the aspiration of ME fluid. Myringotomy involves incising the TM to allow drainage. If fluid is present, its removal will significantly reduce otalgia.
The clinician samples ME fluid for the presence of pathogens. Culturing the fluid and testing antibiotic sensitivity allows the clinician to select an antibiotic appropriate for the specific pathogen.
Tympanocentesis is rarely employed to confirm a diagnosis. There are several reasons for this, including:
Regardless, tympanocentesis should always be performed when AOM is suspected in a neonate. When the immune system is compromised or immature, AOM can become cranial invasive and life threatening.
Myringotomy is not used to diagnose. It is reserved for circumstances when the tympanum might rupture due to severe effusion or purulence. Once myringotomy is performed, the fluid aspirate can be cultured and analyzed for antibiotic sensitivity. Myringotomy involves similar risks as tympanocentesis, along with risk of anesthesia and the possibility of iatrogenic cholesteatoma tympani (cystlike mass associated with chronic infection of the middle ear).
Diagnostic examination
Otologic examination must be performed systematically.
|
Differentiation of AOM from OME is essential to developing an effective treatment plan. |
|
Instant feedback
© RnCeus.com