Fall Risk Factors
Systems theory
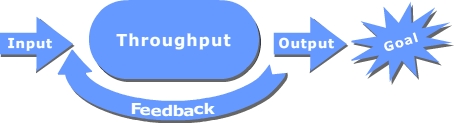
General systems theory originated from the work of biologist Ludwig von Bertalanffy. Any organization can be viewed as a system. The emphasis with systems theory is to see an organization as a whole rather than focusing on individual components. In its simplified version a system can be viewed as input, throughput and outputs with a feedback loop. The entire system is designed to meet goals (Mele et al., 2010).
A systems view is necessary to effectively prevent patient falls. This section of the course describes the patient (input) and hospital environmental factors (throughput) that influence and increase the incidence of falls (Anderson et al., 2013).
Later sections will describe how throughput can affect the incidence of falls.
Input
Patient characteristics that indicate high risk for falls
Patients 65 and older are considered at increased risk of falls even in their own environments. According to the Center for Disease Control (CDC), every year one out of three older adults, 65 and older, experiences a fall. The older the person is, the greater is the risk for falls. The fall rate for adults 85 and older has been reported to be almost four times that for adults 65 to 74. For this age group, falls are also the most common causes of hospital admission due to trauma (CDC, 2015).
In this age group, falls are the leading cause of injury death. The older a person is when they fall, the more likely they are to have serious injuries. The highest rates of deaths from falls, 82%, occur among people 65 and older.
We know according to several research studies the following characteristics contribute to the possibility of a patient falling while in a hospital or other medical facility:
- Age 65 and older
- History of falling
- Confusion, disorientation brought on by disease states or medication
- Diminished ambulation ability
- Dizziness or vertigo
Specific conditions
- A study done in a 1300 bed urban hospital, found the average age of patients who fell was 63.4 years (Hitcho et al., 2004).
- One secondary data analysis of 281,865 high-risk falls assessments identified three factors as strong predictors of falling: history of falls, confusion and taking a laxative (Moe, et al., 2015).
- Osteoarthritis in the lower extremities has been shown to increase the risk of falls. This risk increases with age and associated pain. The arthritis and pain decrease mobility (Zasadzka et al., 2015).
- Anticholinergic drugs have also been associated with increased falls. These drugs block the action of the neurotransmitter acetylcholine in the brain. They are most often used to treat insomnia, incontinence, gastrointestinal cramps and muscular spasms. They are not recommended for elderly patients because of their increased sensitivity to these medications which can cause confusion, memory loss, and other cognitive effects (Zia et al, 2016).
Common uses of Anticholinergic Drugs |
| Indication |
Drugs |
| Parkinson's disease |
- Trihexyphenidyl (Artane)
- Benztropine mesylate (Cogentin)
- Biperiden
- Procyclidine
- Scopolamine
|
| Skeletal muscle relaxant and irritable bowel |
- 2,5 antihistamines (orphenadrine)
- Scopolamine
- Hyoscyamine (Levsinex)
- Belladonna alkaloids
- Propantheline (Pro-Banthine)
|
| Reduce secretions |
- Atropine
- Hyoscyamine (Levsinex)
|
| Urinary incontinence and overactive bladder |
- Flavoxate (Urispas)
- Oxybutynin (Ditropan, Oxytrol)
- Tolterodine Fesoterodine (Toviaz)
- Solifenacin (VESIcare)
- Darifenacin (Enablex) (Mayo Clinic, 2016)
|
- Other medications that are risk factors for falls
Benzodiazepines (example; Valium, Xanax) have been documented as increasing falls and the risk of hip fractures (Passoro, 2000; Rhalimi, 2009). Zolpidem (Ambien) also can cause confusion and dizziness in the elderly particularly (Chang, 2011).
- Gender
The reports describing which gender incurs more falls are mixed with some reporting an increased frequency of falls in males and others and increased frequency in females. One of the issues that makes this determination difficult is the differences in the number of females versus males in the above 65 population. According to the 2010 census females outnumber males at every age junction above 65 with the disparity in numbers increasing in the advanced years.
Throughput – environmental factors
In a study done in a 1300 bed urban hospital found the majority of the falls were unassisted (79%), occurred in the patient’s room (85%) and during the evening/overnight hours (59%). Common in the over 65 year old patients were elimination related falls (50%) with most falls occurring on the way to use bathrooms or in bathrooms. Units with the highest fall rates (6.12 falls per 1,000 patient days) had the highest patient to nurse ratios (5.9 to 1) (Hitcho et al., 2004). Another study reported a decrease in fall rates with units whose nurses had national nursing specialty certification (Boyle, et al., 2015).
Ambulation was also found to increase a time during which falls occurred. This could account for the increase number of falls documented in rehabilitation units (Zhao & Kim, 2015). The number of beds in a room also was a factor in the incidence of falls. In a study of fall rates in single bed rooms versus multiple bed rooms, researchers found an increase in fall rates in the single bed rooms. They have recommendations for not placing elderly patients in single bed rooms (Singh et al., 2015).
Instant feedback
Which of the following have been shown to increase the probability of patient falls occurring?
References
- Mele,C., Pels, J. & Polese,F. (2010). A brief review of systems theories and their managerial Applications. Service Science, 2(1), 126-135.
- Anderson, R. A. (2013). Commentary on "Health care organizations as complex systems: new perspectives on design and management" by McDaniel, Driebe, and Lanham. Adv Health Care Manag. 15, 27-36.
- CDC. (2015). Important Facts about Falls. Centers for DiseaseControl and Prevention, National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention. 1/18/2016 retrieved from http://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html
- Hitcho, E, Krauss, M., Birge, S., Dunagan, W., Fischer, I., Johnson, S. et al. (2004). Characteristics and circumstances of falls in a hospital setting. JGIM: Journal of General Internal Medicine, 19 (7), 732-739.
- Boyle, D.K., Cramer, E., Potter, C. & Staggs V. S. (2015).Longitudinal Association of Registered Nurse National Nursing Specialty Certification and Patient Falls in Acute Care Hospitals. Nurs Res., 64(4), 291-9.
- Moe, K., Brockopp, D., McCowan, D., Merritt, S., Hall, B. (2015).Major Predictors of Inpatient Falls: A Multisite Study. J Nurs Adm., 45(10), 498-502.
- Zasadzka, E., Borowicz, A.M., Roszak, M. & Pawlaczyk, M. (2015). Assessment of the risk of falling with the use of timed up and go test in the elderly with lower extremity osteoarthritis. Clin Interv Aging. 7(10), 1289-98.
- Zia, A., Kamaruzzaman, S., Myint, P.K. & Tan, M.P. (2016). Anticholinergic burden is associated with recurrent and injurious falls in older individuals. Maturitas., 84,32-7.
- Passaro, A., Volpato, S., Romagnoni, F., Manzoli, N., Zuliani, G. & Fellin, R. (2000). Benzodiazepines with different half-life and falling in a hospitalized population: The GIFA study. Gruppo Italiano di Farmacovigilanza nell'Anziano. J Clin Epidemiol. 53(12), 1222-9.
- Rhalimi, M., Helou, R. & Jaecker, P. (2009).Medication use and increased risk of falls in hospitalized elderly patients: a retrospective, case-control study. Drugs Aging. 26(10),847-52.
- Chang, C. M., Chen, M.J., Tsai, C.Y., Ho, L.H., Hsieh, H.L. & Chau, Y.L. et al. (2011).Medical conditions and medications as risk factors of falls in the inpatient older people: a case-control study. Int J Geriatr Psychiatry. 26(6), 602-7.
- Zhao YL, Kim H. (2015). Older Adult Inpatient Falls in Acute Care Hospitals: Intrinsic, Extrinsic, and Environmental Factors. J Gerontol Nurs., 41(7), 29-43.