Glucose Homeostasis
Most animals are obliged to catabolize food and use the freed energy to drive anabolic synthesis. In other words, we consume complex substances, break them down to release energy and we use that energy to fuel, build and repair our own cellular components.
From molds to mammals, glucose is quantitatively the most important fuel source for life on earth. It is the primary fuel for our nervous system and the preferred energy source during initial physical activity. Glucose is also an essential building block for cellular structures. When the body needs to produce lactose, glycoproteins, and glycolipids, they are all synthesized using glucose.
We have two sources of glucose: 1) food, 2) products of metabolism. Food contains carbohydrates, lipids, proteins, etc. Dietary carbohydrates are digested to yield simple sugar molecules in the gut. Simple sugars like glucose, galactose, and fructose pass from the liver's intestinal lumen via the portal circulation. Glucose makes up about 80% of absorbed dietary sugars. Galactose and fructose make up the difference.
In addition to dietary carbohydrates, we synthesize glucose from noncarbohydrate products of metabolism (gluconeogenesis). Gluconeogenesis is particularly essential during fasting and starvation because the erythrocytes, kidney, lens, and cornea depend on glucose as their sole energy source. Glucose is the primary fuel for the brain, but if glucose is low, the brain can switch to ketone bodies to replace about 20% of its glucose requirement. Gluconeogenesis provides the nervous system with a steady supply of glucose even during prolonged fasting.
Glucose is integral to every bodily process. However, the body can store only small quantities of glucose. A total of about 20 grams of glucose are dissolved in the extracellular fluid of an adult. To meet the energy needs during exercise, between meals, and while sleeping, the body stores excess glucose as glycogen or fatty acids.
Adipose, muscle, and liver cells are the primary sites of energy storage. Adipose uses glucose to synthesize fatty acids and triglycerides. Adipose serves as a practically unlimited long term storage for energy-dense lipids. Fatty acids and triglycerides have a metabolic path which is different from glucose and will not be discussed in detail. Suffice it to say that adipose does lower blood glucose levels by absorbing, transforming, and storing it away from the circulating blood.
Muscle stores glucose as glycogen (≈400g), which can be quickly converted back to glucose for muscle activity. The liver can store glucose as glycogen (≈75g) and fatty acids. The liver can also convert stored glycogen to glucose for use by the rest of the body between meals and during fasting and stress. The liver can supply about 16 hours of glucose; after that, other energy sources must be mobilized.
| Adult values |
Fasting Plasma Glucose |
2-hour post glucose test |
| Normal |
<100 mg/dl (<5.6 mmol/l) |
<140 mg/dl (<7.8 mmol/l) |
| Impaired Fasting Glucose |
100–125 mg/dl (5.6–6.9 mmol/l) |
|
| Impaired Glucose Tolerance |
|
140–199 mg/dl (7.8–11.0 mmol/l) |
| Diabetes |
≥126 mg/dl (≥7.0 mmol/l) |
≥200 mg/dl (≥11.1 mmol/l) |
In healthy individuals, insulin-responsive tissues such as adipose, muscle, and liver rapidly absorb glucose to maintain postprandial blood glucose in a fairly narrow range. In individuals with type I and type II diabetes, insulin is either absent or ineffective. The significant actions of insulin include glucose absorption and glucagon suppression. Hyperglycemia can occur when either of these actions is diminished. The 2003 American Diabetes Association - Expert Committee on the Diagnosis and Classification of Diabetes Mellitus has published the following blood glucose thresholds:
GLUT |
| GLUT1 |
All cells |
Low affinity/high capacity |
| GLUT2 |
Liver, B-cells, intestine |
Low affinity/high capacity |
| GLUT3 |
Central & peripheral neurons, placenta, testes, platelets |
Low affinity/high capacity |
| GLUT4 |
Striated & cardiac muscle, fat |
insulin and exercise activated |
| GLUT5 |
Mucus membrane, intestine, sperm |
Fructose carrier |
| The rate of glucose diffusion into the cell is dependant upon the concentration of glucose and the number and affinity of transporters in the plasma membrane. |
Glucose homeostasis requires a continuous balance between glucose diffusion, storage, and metabolism. Glucose cannot enter a cell by simple diffusion. The distribution of glucose across the plasma membrane must be facilitated by glucose transport (GLUT) molecules. The more GLUT molecules embedded in the plasma membrane, the more glucose can diffuse into the cell. The more glucose that diffuses into cells, the quicker the blood glucose level returns to normal.
All cells express GLUT 1 in their plasma membrane. It is believed that GLUT 1 is responsible for basal glucose uptake. Some cells like muscle and adipose can translocate additional GLUT 4 molecules from intracellular storage into the plasma membrane in response to insulin. Like enterocytes in the intestine, other cells can reduce the number of GLUT 2 portals in response to insulin. This has the effect of delaying or reducing dietary glucose absorption. Most cells, significantly in the liver and pancreas, can up-regulate the gene synthesis and expression of GLUT molecules in response to elevated plasma glucose concentration.
 Intracellular glucose concentration must be controlled—low intracellular glucose results in stress and starvation. High intracellular glucose levels have been shown to promote necrotic cell death through H2O2 (peroxide) formation, which may help develop diabetic vasculopathy and associated disease.
Intracellular glucose concentration must be controlled—low intracellular glucose results in stress and starvation. High intracellular glucose levels have been shown to promote necrotic cell death through H2O2 (peroxide) formation, which may help develop diabetic vasculopathy and associated disease.
Mammals coordinate four metabolic processes to regulate intracellular glucose. These processes are glycolysis, glycogenesis, glycogenolysis, gluconeogenesis.
Glycolysis is the enzymatic catabolism of the (6 carbon) sugar glucose into two (3 carbon) molecules of pyruvate + 2ATPs. Glycolysis reduces intracellular glucose which allows additional glucose to safely enter. Glycolysis is a ten step process. Each step is associated with a particular enzyme catalyst. (Click here for the steps). Glycolysis is the anaerobic metabolism of glucose. It is the first step in glucose metabolism and very important during the initial phase of physical activity or when an oxygen deficit limits the body's ability to support good aerobic metabolism.
Glycogenesis is an anabolic process that consumes ATP energy to assemble excess glucose molecules into more complex glycogen granules. A single glycogen granule can contain 30,000 glucose units. Glycogen is synthesized primarily by hepatocytes and muscle. Postprandial glycogen stored in hepatocytes can be as much as 10% of liver mass.
The anabolic hormone insulin initiates glycogenesis. Digestion of food yields glucose, which is transported from the gut to the circulating blood. Elevated plasma glucose causes pancreatic beta cells to release insulin. Increased plasma insulin activates anabolic pathways in the liver, muscle, fat, kidney, and brain. These organs react by 1) facilitating GLUT synthesis, expression, and diffusion of glucose into the cell, 2) increasing glucose metabolism, 3) enhancing the storage of excess glucose, 4) inhibiting the catabolic release of glucose by suppressing the action of glucagon, 5) enhancing lipid production, 6) activating gene cascades that up-regulate cell growth and differentiation. All of these activities have the effect of reducing excess plasma glucose.
Glycogenolysis is a catabolic process that breaks down stored glycogen into glucose. Glycogenolysis provides glucose during short periods of fasting, between meals, during sleep, etc. Glucagon produced in the pancreatic alpha cell, and the adrenal catecholamines epinephrine and norepinephrine are the catabolic hormones that regulate glycogenolysis. Glucagon and catecholamines activate the enzyme glycogen phosphorylase. The liver and muscle are the primary targets of glucagon induced glycogenolysis. Muscle is additionally targeted by catecholamines, which are released during stress and strenuous exercise.
The liver and muscles can absorb large quantities of glucose and store it as glycogen in response to insulin. Between meals, when plasma insulin is low, glucagon increases glucose availability. Glucagon activates the enzyme glycogen phosphorylase, which breaks the bonds holding individual glucose molecules to the glycogen macromolecules stored in hepatocytes and myocytes. In type I and type II diabetes, insulin does not suppress glucagon production. The unopposed action of glucagon in diabetics is responsible, at least in part, for the characteristic hyperglycemia.
Glucose catabolized from glycogen within a myocyte is used only in that myocyte. Glycogen phosphorylase separates glucose from glycogen as glucose-1-phosphate. The presence of a phosphate group at the carbon-1 position makes glucose-1-phosphate too large to diffuse out of the myocyte through a GLUT 4 portal. Glucose-1-phosphate must be converted to glucose-6-phosphate to undergo glycolysis. The enzyme phosphoglucomutase removes the phosphate group from the carbon-1 position and adds a phosphate group to the carbon-6 position. Myocytes can then use the available glucose-6-phosphate in glycolysis or return it to storage as glycogen through glycogenesis.
Hepatocytes, unlike myocytes, produce glucose-6-phosphatase. The enzyme glucose-6-phosphatase can hydrolyze glucose-6-phosphate into a phosphate group and free glucose. A free glucose molecule is small enough to diffuse back to the plasma through a GLUT4 portal. The presence of glucose-6-phosphatase allows the liver to store and release glucose for all body cells. Glucose released by the liver is a primary source of energy between meals. It is also a source of hyperglycemia in insulin-resistant diabetics.
The catecholamines epinephrine and norepinephrine are hormones secreted by the adrenal medulla. These hormones prepare the body for stress like fight or flight activity. Stress hormones also activate the enzyme glycogen phosphorylase. Glycogen phosphorylase breaks the bonds holding individual glucose molecules to the glycogen macromolecule. This provides muscles with the fuel needed for quick sprints and heavy lifts.
A critical factor to consider in the regulation of the rate of gluconeogenesis is the supply of non-esterified fatty acids (NEFA) to the liver. Glucagon and adrenaline also cortisol and growth hormone, compete with insulin and increase hepatic glucose production through an increase in glycogenolysis and gluconeogenesis ( Dimitriadiset al., 2021)
A study by Dufour S. and Lebon V. et al. (2009) demonstrated a 2.5 fold increase of plasma glucose after epinephrine infusion. An inverse association was shown between hepatic glycogen stores and plasma glucose post epinephrine infusion. It was concluded that the majority of hepatic glycogen was converted to glucose in the first 60 minutes following epinephrine infusion and that plasma glucose returned to normal within 90 minutes due to a twofold increase in hepatic gluconeogenesis.
 The liver and kidney express the enzyme glucose-6-phosphatase. These organs use the enzyme glucose-6-phosphatase to remove the phosphate group glucose-6-phosphate. This reaction results in a free glucose molecule and a phosphate group. Free glucose can then diffuse from the cell to the bloodstream.
The liver and kidney express the enzyme glucose-6-phosphatase. These organs use the enzyme glucose-6-phosphatase to remove the phosphate group glucose-6-phosphate. This reaction results in a free glucose molecule and a phosphate group. Free glucose can then diffuse from the cell to the bloodstream.
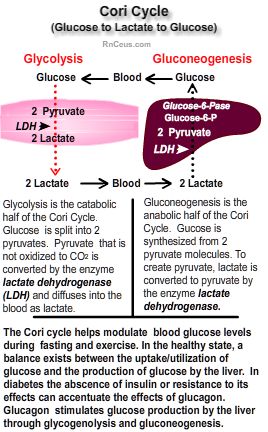
Gluconeogenesis is the synthesis of new glucose from metabolites such as lactate, pyruvate, glycerol, and alanine. For example, lactate formed in muscle and erythrocytes as a metabolic waste product of glycolysis is carried in the blood to the liver, where it is converted to glucose and released back to the blood.
- Type II diabetes mellitus increases the rate of gluconeogenesis. Magnusson and colleagues attribute an ≈18% greater fasting glucose production to gluconeogenesis in people with type II diabetes.
- Type I diabetes increases hepatic glucose production during exercise and at rest. Peterson and colleagues demonstrated that type I diabetic hyperglycemia at rest and during exercise can be entirely accounted for by increased gluconeogenesis. The increased hepatic glucose production during exercise in healthy subjects is the result of glycogenolysis.
- Certain cancers, especially those with rapid cell growth, require large amounts of energy. Glucose production and metabolism are often much higher in these cancer patients than in healthy individuals. J. A. Tayek and J. Katz determined that many cancer patients rely on gluconeogenesis for the bulk of their glucose production. At the same time, healthy individuals derive less than half their glucose by that means.
- G. Bongaerts and H. van Halteren et al. hypothesize, "In growing tumors the O2 concentration is critically low". "In the absence of sufficient O2, they have to switch to anaerobic dissimilation, with only 2 moles of ATP and 2 moles of lactic acid from 1 mole of glucose". "Therefore, growth of these tumor cells will require about 40 times more glucose than it should require in the presence of sufficient O2". "Compensatory glucose is provided by hepatic gluconeogenesis from lactic acid. However, the liver must invest three times more energy to synthesize glucose than can be extracted by tumor cells in an anaerobic way. The liver extracts the required energy from amino acids and from fatty acids in an oxidative way. This may account for weight loss, even when food intake seems adequate".
Instant Feedback:
Insulin causes the liver and muscles to absorb glucose and store it as glycogen.
References
Bongaerts, G. P. A., van Halteren, H. K., Verhagen, C. A. M., & Wagener, D. J. Th. (2006). Cancer cachexia demonstrates the energetic impact of gluconeogenesis in human metabolism. Medical Hypotheses, 67(5), 1213–1222. https://doi.org/10.1016/j.mehy.2006.04.048
Dimitriadis, G. D., Maratou, E., Kountouri, A., Board, M., & Lambadiari, V. (2021). Regulation of Postabsorptive and Postprandial Glucose Metabolism by Insulin-Dependent and Insulin-Independent Mechanisms: An Integrative Approach. Nutrients, 13(1), 159. https://doi.org/10.3390/nu13010159
Dufour, S., Lebon, V., Shulman, G. I., & Petersen, K. F. (2009). Regulation of net hepatic glycogenolysis and gluconeogenesis by epinephrine in humans. American journal of physiology. Endocrinology and metabolism, 297(1), E231–E235. https://doi.org/10.1152/ajpendo.00222.2009